WHO Reform 2010-12
Full WHO Watch Report on WHO Reform now available for download
- Background - what it is all about
- Current issues - where you can make a difference
- History - a detailed history of the current reform program
- Key issues - a summary of some of the key issues at stake
Background
The World Health Organisation is a critically important global institution. It has a unique role to play in addressing the health needs of people around the globe, vulnerable populations in particular.
But WHO is today in crisis. For over thirty years the rich countries have sought to control the Organisation by refusing to fund the priorities of the membership as a whole while selectively funding those programs which are consistent with their interests and perspectives. Generous funding is supplied to projects which are designed in part to protect the intellectual property rights of European and US pharmaceutical giants while programs directed to the effective and efficient use of medicines and quality of care are seriously underfunded. Health system development is one of the critical areas of work in developing countries and WHO has taken the lead in promoting universal health care, integrated health systems and primary health care. However, the World Bank promotes a stratified model of health care (private for the rich, social insurance for the middle and safety nets for the poor) and the Global Fund for AIDS, TB and Malaria promotes a vertical fragmented model of health care focused solely in three priority diseases. However, adequate funding is not available to WHO to promote integrated, PHC based health care. (See Walt (1993). "WHO under stress: implications for health policy." Health Policy 24: 125-144 for an early analysis of the unfolding crisis.)
In a Catch 22 twist, the funding crisis has contributed to undoubted inefficiencies in the work of WHO which are then taken as the reason for not untying its funding.
The issue of WHO Reform was re-opened for official discussion at the May 2009 World Health Assembly (WHA) when the focus of concern was WHO's increasing dependence on earmarked funds from donor countries and foundations. Since then the range of issues at stake has been widened to encompass a broad approach to WHO reform. Meanwhile different parties with different agendas are seeking to drive the reform in different directions. This increasing complexity is reflected in the increasing number of technical papers prepared by the Secretariat for each meeting of the Executive Board (EB) & the World Health Assembly (WHA).
Current focus
At the time of writing (mid August, 2012) the forthcoming discussions where decisions may be made include:
- regional committees, from 4 Sept to 26 October;
- the extraordinary meeting of the Programme, Budget and Administration Committee of the EB (PBAC) from 6-7 Dec 2012 and
- the 132nd EB from 21-29 Jan 2013.
The regional committees are expected to consider, amongst other things, the draft Global Program of Work 2014-19 (GPW12), the draft Programme Budget 2-14-15 (PB14-15) and the proposals listed in WHA65/5 for reform including proposals for 'closer alignment' (lining up the work of countries, regions and headquarters) and 'harmonisation' (bringing some closer standardisation to the procedures and structures at the regional level).
One of the critical issues to be considered in connection with the draft GPW12 will be the reduced set of categories and the fate of the so-called cross cutting issues such as social determinants of health, gender equity, health as a human right and primary health care. Concern was expressed by many MS during WHA65 regarding a perceived downgrading of these issues and the risk that they would be sidelined. See WHO Watch report of this discussion.
Among the decisions of the 'MS driven process' of Feb 2012 was a commitment to a web-based consultation around the draft Twelfth General Programme of Work 2014–2019 in order 'to solicit input and comments from a wider group of stakeholders' to be held from mid August to mid October 2012. Arrangements for this consultation have not yet been posted.
The extraordinary meeting of the PBAC (Dec 6-7, 2012) will consider "options developed pursuant to document A65/5 of the Sixty-fifth World Health Assembly on transparency, predictability and flexibility of WHO’s financing (see paras 93-95); and review of the issues raised by discussions in regional committees concerning the draft Twelfth General Programme of Work and the Proposed programme budget". This will be a critical decision point because the 'modalities' of the proposed 'funding dialogue' will be considered and recommendations developed for the EB in Jan 2013.
EB132 in Jan 2013 will adopt a draft GPW12 and a draft PB14-15 which the DG will then take to the funding dialogue. The EB132 will also adopt the guidelines (modalities) for the conduct of the funding dialogue. The DG will then go out seeking donor support for the priorities adopted by the EB and a final PB14-15 will be presented to the WHA66 (May 2012) based on priorities developed by the EB as selected for funding by the donors. This situation epitomises in concrete form the reality of donor control of WHO's budget.
The EB will also develop recommendations for the WHA66 on other aspects of WHO reform including relationships with the private sector and with civil society and the conduct of 'partnerships'.
Meanwhile a number of strands of the reform program on which decisions have already been taken are proceeding to implementation within the Secretariat (see Decision WHA65(9)). These include implementing the new evaluation policy, implementing the new 'results chain', improving the quality of WHO representatives at the country level, reshaping the staffing body (the balance between permanent and project staff and the balance between levels) and reshaping expenditure patterns as between headquarters, regions and countries.
History of WHO Reform Discussion
WHO funding and reform have been discussed repeatedly over many years. John Farley ('Brock Chisholm, the World Health Organisation and the Cold War'. Vancouver, UBC Press, 2008) describes a recurring tension between the 'have' nations and the 'have not' nations over the level of 'assessed contributions' from the earliest years of the WHO.
In 1994 a study of WHO revenues was commissioned which confirmed that even at that stage WHO was slipping into a funding crisis. Further details.
WHA61 (May 2008) discussed a significant funding gap between the PB08-09 and the available revenue for the biennium, in particular for basic administrative functions (see A61/41) and agreed to transfer a surplus (arising from exchange rate movements) in miscellaneous income from 06-07 to 08-09 (see WHA61.6). At this meeting Canada, US and NZ commented on the refusal of some donors to provide the 13% overhead charge with their donation with the consequence that assessed contributions funding was entrained to subsidise donor funded projects (see report of Committee B discussion, p192).
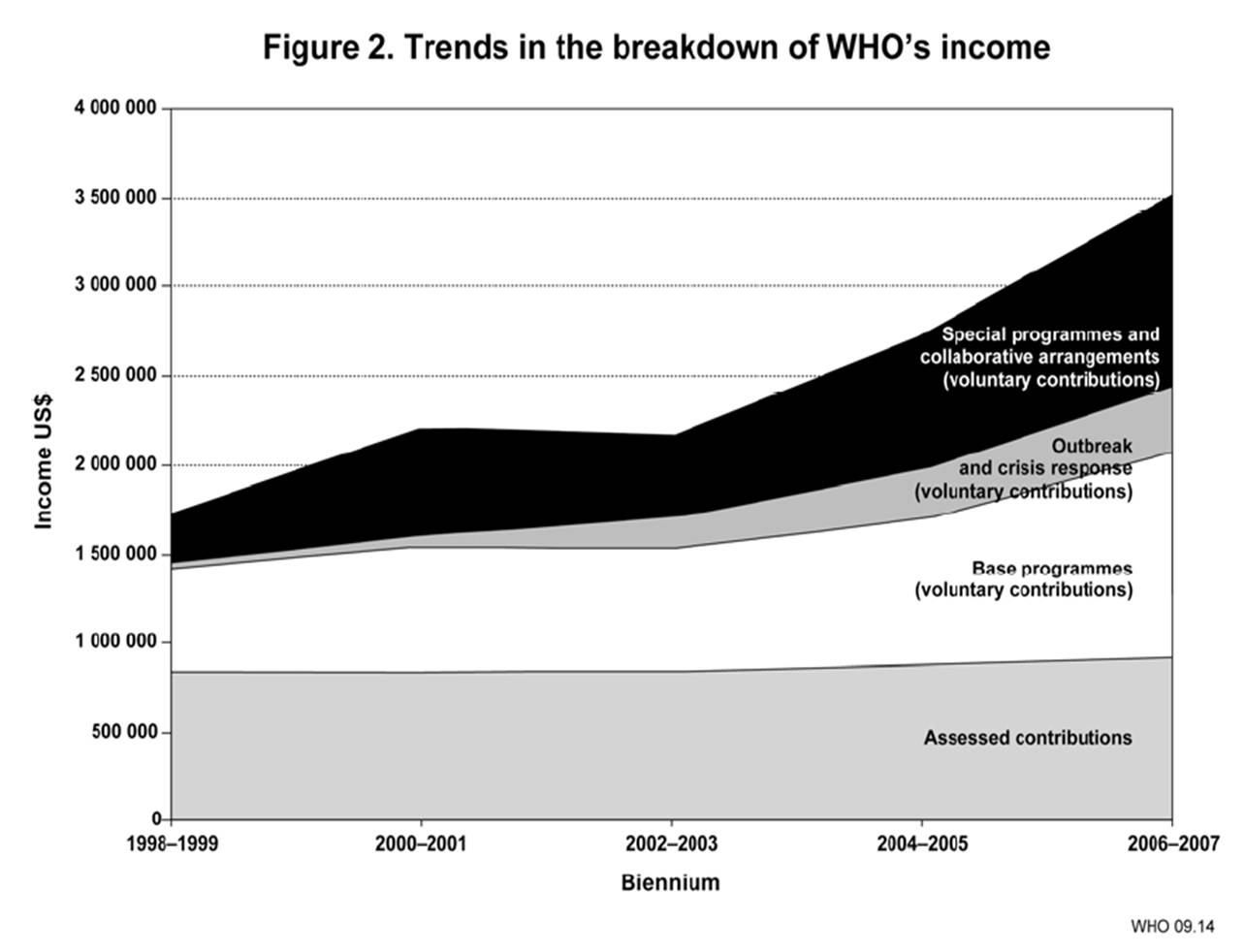
The underlying financing issues were reviewed at EB124 (Jan 2009) where the Secretariat tabled a revised MTSP2008-2012 and a proposed PB2010-11 (EB124/20). The commentary introducing the revised MTSP demonstrated that assessed contributions had been kept constant while earmarked funds had been increasing. See Figure 2, Trends in the breakdown of WHO's income, at para 68 in the Revised MTSP (discussed EB124 in Jan 2009 and adopted WHA62 in May 2009). (At this stage income was being analysed in terms of its flow into 'base programs', 'special programs and collaborative arrangements' and 'outbreak and crisis response' (see definitions in the Introduction to the proposed PB10-11).
During EB124 both the Secretariat and member states expressed concern about the disproportionate patterns of funding with certain high priority areas (eg NCDs) being underfunded while others were attracting open flows of voluntary donations. The revised MTSP08-13 and the proposed PB10-11 were discussed in the PBAC and then at the EB. See record of this EB discussion (page103). During this discussion the policy of 'zero nominal growth' in assessed contributions explicitly re-affirmed by Hungary for the EU, Canada and Japan. The revised MTSP and PB10-11 were discussed and adopted as amended at WHA62 (May 2009). See record of discussion (from p50)
In response to the concerns about the distortion of MS priorities arising from the unbalanced funding structures, the Director-General convened an informal discussion in January 2010 followed by a web consultation between April and October and further discussion at the regional committtes in late 2010.
For EB128 (Jan 2011) the DG tabled a report to the Board (EB 128/INF.DOC./2) summarising the views of Member States (MS) and the issues raised. The DG also prepared a report to the EB on the Future of Financing of WHO (EB128/21) for the consideration of the EB128.
{kind=link}
What became clear in the consultation was that there was no enthusiasm among the MS to increase assessed contributions (ACs) or even among the LMICs to put pressure on the HICs to increase their contributions. As a consequence the discussion about funding moved from increasing ACs to shifting the balance in donations from tied to less tied and finding new sources of funds (which the DG indicates includes the BRICS, private foundations and the private sector).
However, one of the messages emerging from the consultation was also about cutting back on what WHO does and this message was tied to a number of other themes (priority setting, results focus, global health governance, partnerships, personnel reform, and organisational coherence).
The discourse of 'priority-setting' entrains further streams including 'live within your means', '[only] do what WHO does best', and 'partnership' as in 'work in closer partnership with the various global health initiatives (GHIs)'. The discourse of 'results' entrains ideas about the need to demonstrate efficiency and effectiveness, through more rigorous evaluation protocols and practices. The discourse of 'global health governance' links to the discourse of partnerships: WHO has a role in norm-setting and convening but perhaps should invest less in technical assistance; work more in 'partnership' with the GHIs and other 'stakeholders'.
The need to review organisational design was not so clear from the consultation report but was emphasised by the DG in her commentary. Presumably her concerns include reining in the independence of the regions and clusters.
The need for personnel reform is also an issue emphasised by the DG in her report, partly in connection with the staffing of country offices and partly as a more general issue of organisational flexibility and the need for a staffing model which supports such. One of the issues here is about the balance between permanent staff and contract staff but it also includes questions about the quality of staff, in particular at the country level and the distribution of staff resources between the three levels of the Organisation.
In introducing the discussion at the Jan 2011 EB (see the official record of the discussion at the Sixth Meeting of the EB) the DG listed the six elements of her report (EB128/21). She eleborated on her notion of a multi-stakeholder forum which she presented as a development of WHO's global health governance responsibilities. Highlights from the discussion of this item at the EB were the contributions of the US who asked for clarification of the idea that WHO might have an advocacy role in public health and India who emphasised the dangers to the Organisation from the dominance of earmarked donor funding. No formal decision was taken but there were expressions of support for the DG in progressing the reform program.
The DG summarised what she took from the discussion in her concluding remarks (EB128/INF.Doc./3) and indicated that she would prepare a 'programme of reform' which she would bring to the WHA64 (May 2011).
Following EB128, an informal consultation was convened in Geneva on March 11, 2011. See the PHM/MMI report of March 11 consultation. Much of the focus of this discussion was on the proposed World Health Forum which was presented as WHO taking a more forward position in relation to global health governance.
The papers prepared for discussion at the WHA64 (May 2011) included a revised version of 'The future of financing' (Document A64/4) and a more practical 'development plan' (WHA64/INF.DOC./5). These built upon the the discussion at the January 2011 EB, the March 11 Consultation, and discussions on the side lines of the April 2011 Moscow Ministerial meeting on NCDs.
A64/4 starts with a focus on WHO's 'core business' which it discusses in terms of five functions: convening for better health, generating evidence, providing advice, coordinating health security and strengthening health systems and institutions. The paper then proceeds to outline the six main streams of work to be undertaken as part of the reform program: organisational effectiveness, results based management, personnel reform, financing and resources, effectiveness at country level and strengthening WHO's role in GHG.
Document WHA64/INF.DOC./5 sets out expected outcomes and outputs associated with six main streams of reform work. The outputs reflect the main strategies to be deployed to achieve the outcomes. Thus the sole strategy for improving WHO's effectivenss at the country level is an enhanced recruitment and assessment mechanism for Heads of WHO country offices. Some of this material is quite obscure, eg the strategies for 'increasing organisational effectiveness'.
The issues listed in A64/4 were discussed in May 2011 at WHA64 (see official record of discussion during the 3rd meeting of Committee A).
Many of the contributions were cast in general terms, supporting the DG and agreeing broadly with the need for better priority setting and for WHO to play its proper role in global health governance. The Thai contribution (p6) was a standout in terms of frankness. The EU, UK and France spoke about the importance of WHO living within its current budget through more disciplined priority setting. India (p14) regretted the lack of detail, was surprised at the call for a World Health Forum and urged more discussion and deliberation. (See WHO Watch comment on A64/4.) In the end Resolution WHA64.2 which broadly endorsed the DG's development plan was adopted.
The EB129 (in May 2011, immediately after the WHA64) reviewed progress on WHO Reform. See WHO Watch report of this discussion and Decision EB129(8) on WHO Reform. This decision requested the DG to prepare discussion papers on: governance of WHO, independent evaluation of WHO, and the proposed World Health Forum. The EB requested further consultation on these papers through a web-based platform and in the regional committees and then an open meeting in special session of the Executive Board in November to further the discussion.
In July 2011 the WHO Secretariat released three concept / discussion / decision papers on: the Governance of WHO, a proposed Independent Formative Evaluation of WHO's work (which might focus as a kind of first step on HSS and/or possibly MCH); and the proposal for a new structure, a World Health Forum (as called for in Resolution WHA64.2). From August to November these papers were subject to further consultation and revision including a web-based consultation and face to face discussion at the six regional committees which met from August through to October.
In October 2011 the DG circulated a new version of WHO Reforms for a Healthy Future (15 October) building on and incorporating comment on the three earlier discussion papers as well as a new Road Map for organisational review and reform for discussion at the special session of the Executive Board (EBSS) in November 2011. The EBSS adopted three decisions, dealing respectively with programme definition and priority setting; with governance (both of WHO and WHO's role in), and managerial reform.
On Programmes and Priority setting (EBSS2(1)) the Board commissioned and specified a further discussion paper and planned a 'member-state-driven process' which turned out to be a two day meeting in Geneva in February 2012. The purpose of this process would be to recommend 'methods for programme and priority setting' to the WHA65 (May 2012).
On Governance (EBSS2(2)) the Board agreed to a set of governance principles; decided to strengthen the role of the PBAC in WHO governance; decided to explore re-scheduling of the Programmme Budget and Administration Committee of the EB (PBAC) and EB sessions; proposed limits on draft resolutions coming to the Assembly; proposed tighter disciplines with respect to speaking times; called for further attention to the links between regional committees and the EB & WHA; called for more support to member states (MSs) in preparing for governing body discussions; called for a strengthening of dialogue and engagement with stakeholders; and affirmed the leadership role of WHO in global governance for health. The Decision requested the DG to prepare revised terms of reference for the PBAC (for EB130 in January 2012) and called for further analysis and proposals for the other items listed.
On Managerial reform (EBSS2(3)) the Board adopted a complicated and somewhat confused Decision which:
- authorised the DG to take forward her reform proposals in several identified areas but urged caution in relation to two of the areas identified;
- requested further papers to be prepared for EB130 in Jan 2012 on flexibility of funding; funding for public health emergencies; evaluation policy; relations between the different levels of the organisation;
- requested a proposal for a new resource allocation mechanism to go to the PBAC in May 2012;
- requested a proposal regarding the development of the GPW12 (14-19) and PB (14-15) for WHA65 in May 2012;
- and decided to proceed with a two stage evaluation as an input to the reform process .
See NGO Comment on EBSS Decisions (111205).
WHO reform was considered again at the EB130 in Jan 2012. On this occasion the EB had before it nine documents in addition to the decisions of the EBSS. These documents included a general overview report (EB130/5 WHO reform) which summarises the nine, more specific documents. The EB elected to consider these documents in three groups as follows:
- 1. Programmes and priority setting (see WW report of discussion)
- EB130/5 Add.1 Programmes and priority setting (see WW comment)
- EB130/5 Add.2 Distribution of financial and human resources (see WW comment)
The Board's decisions on this item are contained in its formal decision (EB130(6) WHO reform (programmes and priority setting)) and the Chairperson's Summary of decisions on WHO Reform which records that Programmes and Priority Setting will be discussed at the special MS process (meeting) scheduled for 27 and 28 Feb 2012. Decision EB130(6)specifies the objectives of the 'MS driven process' (largely focused on categorisation of WHO's work and methods for setting priorities); and specifies the documents to be prepared by the Secretariat for the meeting in Feb: a review of current priority setting processes; a mapping of the functions of WHO; an analysis of country cooperation strategies and timelines for the preparation of the GPW12 and PB14-15.
- 2. Governance (see WW report of discussion)
- EB130/5 Add.3 WHO Governance (see WW comment)
- EB130/5 Add.4 Governance: stakeholders and partnerships (see WW comment)
The Board's considerations of these papers are referred to in the Chairperson's Summary of the Board's decisions on Governance. These include revision of the terms of reference of the PBAC; increasing alignment of the work of the different levels of WHO and increased harmonisation of the methods of working of the different regions. The Chairman foreshadows revision of the current schedule of meetings of the governing bodies; further discussion of relationships with various different kinds of stakeholders (NGOs, private sector and foundations) and further consideration of 'partnerships'.
- 3. Managerial reforms (see WW report of discussion which included
-
EB130/5 Add.7 Organizational effectiveness (see WW comment)
-
EB130/5 Add.9: Managerial reform: evaluation (see WW comment)
Finally the Board considered strategies for progressing the consideration of WHO Reform in the governing bodies (see WW report of this discussion). The Chairperson's Summary records a commitment by the Secretariat to prepare a consolidated report of all aspects of WHO Reform to be considered during the May 2012 meetings of the governing bodies.
In February 2012 the special meeting of member states focusing on priority setting was held in Geneva. The purpose of the meeting is articulated in the decision of the EB130 in Jan 2012 (EB130(6), page7) which decides to hold a MS process on Feb 27-8 to discuss EB130/5 Add.1, looking at priority setting and the categorisation of WHO functions and evaluation. The EB Chairperson's summary of the Board's consideration of WHO Reform provides further detail regarding the purpose of this meeting.
The EB decision of Jan 2012 (EB130(6)) regarding priority setting commissioned the Secretariat to produce the following papers for the February 2012 MS meeting:
-
Document 1 on programmes and priority Setting provides a detailed review of the existing planning tools including the GPW, the PB, the MTSP and the terminologies which have been developed in working with these tools. a review of the context, issues and options regarding priority setting; it offers some observations about priority setting and refers to a suggested methodology;
-
Document 2 provides a mapping of the functions of the Organization; first mapping the categories proposed in document EB130/5 Add.1 against the functions articulated in Article 2 of the WHO Constitution) and second, against the strategic priorities in the current GPW, including crosscutting global needs;
-
Document 3 reports on an analysis of country cooperation strategies, listing the frequency with which particular categories of work and functions are identified as priorities in the CCSs; it is presumed that the frequency with which particular priorities are identified provides some indication of what WHO should focus on and where WHO is thought best placed to add value; see further information on country cooperation strategies;
-
Document 4 provides a road map and timelines for the preparation of the Twelfth General Programme of Work and the Programme budget 2014–2015.
There were no decisions or resolutions out of the February meeting but the Chairman of the meeting penned a Chairperson's Summary of the views of the meeting on which was submitted to WHA65 as Doc A65/40. The Chairperson's summary offers:
- a set of criteria for setting priorities;
- a set of categories 'for priority setting and programmes';
- a road map and timelines for the development of and consultation around the GPW12 and PB14-15
Interestingly the location of the financing dialogue with donors (between the EB in January and the WHA in May) is NOT highlighted in the Chair's summary of events and timelines.
Among the decisions from this MS driven process, as formulated by the Chairperson, was a commitment to a web consultation around the draft Twelfth General Programme of Work 2014–2019 in order 'to solicit input and comments from a wider group of stakeholders' to be held from mid August to mid October 2012. Arrangements for this consultation have not yet been posted (as of 21 Aug, 2012)
These various issues were further considered in May 2012; by the PBAC (18 May), by the Assembly (WHA65, 21-26 May) and then by the EB (EB131, May 29-30).
WHA65 (May 2012) had before it six key documents:
-
WHO Reform. Consolidated report by the DG (Document A65/5)
-
Draft Twelfth General Program of Work and explanatory notes (Doc A65/5 Add.1)
-
Independent Evaluation Report (Stage 1), presented by the External Auditor (A65/5Add. 2),
-
Draft Evaluation Policy for EB131/3
- Report by the Chairman of the meeting of Member States on programmes and priority setting 27 to 28 February 2012 (Doc A65/40)
- PBAC report to WHA65 (A65/43).
The WHA agenda presented three groups of issues to the Assembly: WHO reform, a first draft outline of the GPW12 and the Stage I Evaluation Report.
The DG's Consolidated Report (A65/5) (CR) on decision making and progress with respect to WHO Reform was structured around 16 ‘decision points’ for decision by the Assembly. See WW comment on A65/5.
The draft outline of the 12th Global Program of Work for 2014-19 (GPW12) (Document A65/5 Add.1) was presented first to the PBAC and then considered by the Assembly. (A more detailed version, with a first draft Programme Budget 2014-15 (PB), has since been posted (Aug 2012) for consideration first, by the regional committees in late 2012; then by the extraordinary meeting of the PBAC in December 2012 and then to the EB in Jan 2013 and then for final adoption by the Assembly in May 2013.) The draft outline GPW12 (May version) was scheduled for discussion with the DG’s Consolidated Report on WHO Reform because it sought to operationalise the principles developed in the WHO Reform discussions, in particular those regarding priority setting. See WW comment on the May draft of GPW12.
Finally the WHA considered the report of the Stage I Evaluation of the WHO Reform Program (A65/5Add. 2). One of the papers prepared in July 2011 had dealt with evaluation; this paper was then reworked for the EBSS WHO Reforms for a Healthy Future (15 October) . See the decision of the November EBSS regarding this evaluation in EBSS2(3).
The terms of reference for the Stage 1 Evaluation adopted by the EBSS in November focused on the assembly of management information relevant to the evaluation of WHO. Following the MS driven process in Feb 2012 the terms of reference were rewritten by the Secretariat to focus the evaluation on the WHO reform process. WHA65 was invited to note the findings of the Evaluation Report (A65/5 Add.2) and recommendations, as well as the Roadmap for Stage II. See WW comment on the Evaluation Report.
- categorisation of programmes,
- formulation of the GPW12,
- governance reforms (including sequencing of governing body meetings, aligning the work of RCs with that of the EB, harmonising the procedures of regional offices (including the presence of observers at RC meetings), streamlining governing body meetings, and policy development around relations with NGOs) and
- managerial reforms (including personnel reform, the funding dialogue, conflict of interest, evaluation, and strategic communications).
Following the WHA65, the EB131 gave further consideration to WHO Reform, including amongst other items
- a presentation from the representative of the WHO staff associations which included extended comment on the disabilities and directions of the Secretariat; and
- the report of the PBAC16 (held just before the Assembly).
The EB further progressed some of the WHO Reform streams of work:
- adopted revised terms of reference for the PBAC;
- adopted the revised Evaluation policy (EB131/1) as presented
- decided (EB131(10)) to hold an extraordinary (open to all MS) meeting of the (newly empowered) PBAC from Dec 6-7, 2012.
" ... which would focus its agenda on: particular aspects of WHO reform; consideration of options developed pursuant to document A65/5 of the Sixty-fifth World Health Assembly on transparency, predictability and flexibility of WHO’s financing; and review of the issues raised by discussions in regional committees concerning the draft Twelfth General Programme of Work and the Proposed programme budget;"
Thus the key issues for consideration at this extraordinary PBAC meeting will be:
-
the Global Program of Work 2014-19 (see current draft in development for regional committees) and the Program Budget 2014-15
-
the modalities for the proposed Funding Dialogue
The PBAC will meet after the last of the Regional Committees has met and will have some material from these meetings. It is not clear how much the PBAC will get into the substance of the GPW and PB or will focus on the structure of these two documents and the relationships between them and the processes of progressing them. The scheduling of the funding dialogue and the structures and procedures also remain very unclear. Decision EB131(10) requests the DG:
"(5) to provide, as part of the preparations for its 132nd session and for the Sixty-sixth World Health Assembly, briefings for Member States on all aspects of reform implementation, ensuring that the relevant documentation is available at least 10 days before the start of the extraordinary meeting of the Programme, Budget and Administration Committee in December 2012, and before the 132nd session of the Executive Board in January 2013;
(6) and to submit a document to the Executive Board at its 132nd session that identifies and assesses specific options on the elements set out in document A65/5, in particular on WHO internal governance, including the alignment of headquarters, regional and country offices on the issue of WHO’s role on global health governance, and the methods of work of the governing bodies."
Key themes of the WHO Reform Debate
Funding and priority setting
The mismatch between the priorities identified in resolutions of the WHA and the amount of funding available to the Secretariiat remains at the heart of the 'WHO Reform' debate. Assessed contributions have been capped since the 1980s with a progressive increase in voluntary contributions to around 80% of total expenditure. Essentially the rich countries refuse to allow for appropriate growth in flexible (untied) funding (through assessed contributions) but are willing to support specific programs through tied voluntary contributions. Under Gro Harlem Brundtland the clusters and regions were actually encouraged to take a more entrepreneurial approach to seeking donor funding leading to a dysfunctional decentralisation of management to the independent fiefdoms of Cluster Geneva and the regional directorates.
This was the situation which Dr Margaret Chan inherited in 2006 so it is not surprising that she opened the debate under the rubric of 'The future of financing of WHO' which was the title she gave to the report of the 2010 consultation and to the report submitted to EB128 in Jan 2011. Note the comments in A64/4 of May 2011:
"74. Flexible funding remains an essential component of reform, in that it can enable WHO to respond more effectively to new health challenges and a changing environment. Flexible funding is also a potential outcome of the reform process, on the assumption that greater confidence in WHO’s policies and practices, and the implementation of the reforms set out in this report, will enable more donors to fund the Programme Budget as it stands.
75. In reality, many voluntary contributions will continue to be specified. More transparent priorities, deliverables and the process of resource allocation can reduce this problem by facilitating the alignment of specified contributions with corporate priorities. However, when looking to the future, alignment will always be difficult to achieve if less than a quarter of the Organization’s funding is predictable and flexible. For this reason, Member States are urged to give serious consideration to the issue of increasing assessed contributions and, where appropriate, revisiting national policies that restrict their growth."
The amounts of money contributed as voluntary contributions varies widely among members. Calculations (see tables) based on A65/30 and A65/29 Add.1 show that VCs from the top 10 MS contributors constitute 223% of their ACs whereas VCs from other MS in total constitute only 37% of total (other MS) ACs. Even among the top 10 contributors this ranges from Norway (VC=14.8xAC) and Australia (VC=5.9xAC) to Japan and France whose VCs amount to only 40% and 41% of their ACs. VCs from the BRICS vary from 11% of ACs (China) to 86% (Russia).
In terms of untied versus earmarked donations the top 10 MS vary widely also from Spain and Norway which provide 53% and 42% of their total VCs as untied 'core VCs' compared with the US, Canada, Japan, France, Germany which provide none of their VCs as untied core. None of the BRICS contribute any of their VCs as core / untied.
The report of the 2010 Consultation and later discussions in the governing bodies suggest that most MSs are not willing to confront the problem of capped ACs and are not willing to recognise how the growth in donor control (and the emergence of the fiefdoms) had compromised the effectiveness and efficiency of the Organisation as a whole. Instead the basic message appears to have been about priority setting: that WHO "cannot sustain the diversity of its current activities, and must select fewer priorities". Rather than providing more funds to meet contemporary global health WHO is asked to 'live within your means' essentially do less with less.
'Priority setting' has remained a leading theme in the discussions of WHO Reform. Following this logic the Organisation has been asked to reconceptualise its role (its 'core business') in the 'crowded landscape of global health architecture' as one approach to identifying priorities. The implication, that WHO's financial woes arise from some kind of overlap or competition with the plethora of global health initiatives which have emerged over the last decade, is highly contentious.
There has been much talk about priorty setting, a results chain and outcomes and ouitputs but the Organisation (both Secretariat and MS) have been much more uncertain in terms of developing a robust methodoiogy for priority setting. The current version of the GPW12 documents the methodology in use. MS expressed concern at both at WHA65 and EB131 over the risk of losing the 'cross cutting issues'; MS were particularly concerned about social determinants of health. These concerns are acknowledged in the c
Three further themes which have emerged under the rubric of 'priority setting' are: (i) WHO's role in global health governance; (ii) WHO's intrinsic 'competitive advantages'; and (iii) 'partnerships'. The discourse of 'returning to WHO's core role in GHG' means that WHO should restrict itself to its 'normative' role (the first curtain of fog) which means restricting it to developing standards for vaccines or rules for responding to epidemics. The discourse of 'competitive advantage' means that WHO should restrict itself to convening meetings and publishing manuals.
The discourse of 'partnership' is an indirect way of restricting WHO to technical norm setting and leaving 'implementation' and technical cooperation to the GHIs, global foundations and the World Bank. Despite repeated requests from MS the Secretariat has been quite coy about publishing the full list of 'partnerships' and documenting the purposes, activities, governance and funding of these partnerships. A commitment has been made to reporting on those partnerships which are hosted by WHO but no such commitment has been made regarding the full suite of partnerships.
Another counter-discourse in discussions of WHO financing has been the idea of 'innovative funding' which is code for 'broadening the donor base' and 'attracting more funds from the private sector'. See A65/29 Add.1 for current private sector donations.
Efficiency and effectiveness
WHO is probably not the most efficient nor effective organisation in the UN system but the argument that funding should be contained as a means of encouraging improved efficiency and effectivenss is spurious.
The most basic restriction on WHO efficiency is its democratic base. Every decision of WHO, from the policy decisions of the governing bodies to the operational decisions of country representatives, involves compromises; compromises over objectives, strategies and outcomes; compromises which are reflected in funding arrangements and in the politics of implementation. Many of these compromises reflect the changes in global power structures from post-war colonialism to the emergence of the BRICS. Every increment of change is resisted and such resistance is reflected in compromise.
Efficiency and effectiveness call for clarity with respect to objectives and selection of strategies directed to those objectives in the most efficient and effective way and implementation supported by monitoring evaluation and feedback so that adjustments to improve efficiency and effectivenss can be made. In a body like WHO there are intrinsic barriers to achieving this kind of coherence between objectives, strategies and operations.
Some of these disabilities were embedded in the original design of the WHO, in particular, its highly decentralised structure. This decentralisation is a limit on efficiency but could be a powerful force for effectiveness. The missing ingredient is accountability to civil society. The regional directorates are largely accountable to the ministries of health, certainly not to the people they are supposed to be working for. When the ministries of health and the regional directorates are more transparent and accountable to the people they are supposed to serve, the decentralisation of WHO will transform from disability to asset.
A further disability arises from the staffing structure of WHO and the compromises which have been made over the years to negotiate the changing workforce environment in order to deliver on the promise of the Constitution. The objective of geographic equity in staffing conflicts with an unequal global distribution of financial and human resources. This is a reality which can only be managed through compromise with costs in terms of efficiency and effectiveness. However, the balance is changing and the tension must be managed creatively across the dynamic of change.
However, notwithstanding these structural disabilities, the main source of inefficiency and ineffectiveness in the present period is the chokehold of the donors. The present DG inherited a federation of competing fiefdoms who under Gro Harlem Brundtland had been encouraged to compete with each other in attracting funds from (and servicing the interests of) the donors. This created a seriously dysfunctional and strategically incoherent organisation. The future of the WHO depends on the restoration of member state sovereignty, even at the cost of losing large scale donors.
Accountability, transparency, evaluation
Alongside accusations of ineffieciency and ineffectiveness, accusations of lack of accountability and lack of transparency are trotted out as reasons why the chokehold should not be loosened. But accountable to whom?
Both Secretariat and MS frequently repeat the statement that WHO is an intergovernmental organisation, a MS driven organisation. This suggests that it should be accountable to MSs. However, the accountability of MS to their own governments and people for their conduct as members of WHO is in many cases quite limited and subject to distortions.
The most obvious distortion of accountability is the donor chokehold. The Secretariat is accountable to the donors and potential donors in a much sharper way than it is accountable to MSs.
Many delegates to the Assembly have not read the papers and have not fully considered the issues before the Assembly at the national level before attending. The positions adopted by many of the big powers are in some cases more directed to protecting the interests of their own transnationals, in particular, big food and big pharma, than promoting the health of the people. Delegates and MS health ministries have very limited accountability for how they govern WHO.
This discussion of accountability raises two linked issues: conflicts of interest and the role of civil society in strengthening the democratic accountability of WHO and MS representatives.
WHO has long had formal COI protocols for the professional experts who sit on its committees although these protocols have been breached in some failrly high profile cases. But institutional conflicts of interest have been widely ignored until recently. See the IBFAN Consumers International statement on Conflict of Interest at the WHA65 in May 2012.
Civil society has a powerful role to play in supporting WHO and also strengthening its accountability and the MS representatives. WHO, both MSs and Secretariat have been very cautious about facilitating such a role.
Staffing profile and policies
Staffijng issues are highly relevant to the efficiency and effectiveness of WHO. We shall post a more detailed analysis shortly. Some key recent documents include:
- report of external auditor (A65/32);
- report of the internal auditor (A65/33)
- human resources: annual report (A65/34)
- report of international Civil Service Commission (A65/35)
- statement to EB131 by representative of WHO staff associations
| Attachment | Size |
|---|---|
| Legge110909_WHOReformBackgroundOptions.pdf | 598.09 KB |
| DGHLetter2MS_110630.pdf | 565.2 KB |
| DGHLetter2UNMissions_110914.pdf | 111.94 KB |
| TWN_110916_CommentOnWHOReformPapers.pdf | 97.25 KB |
| DGH&PHMCommentEBSS-Decisions_2011-1205.pdf | 157.67 KB |
| ACs&VCs(2010&2011)_120822A.pdf | 102.85 KB |
| WHOWatch(120831)ReportWHOReform.pdf | 155.13 KB |
| Fig2BreakdownWHOIncome2009.jpg | 64.83 KB |
| 3_WHOHistory&GHPolicy_IPO(2014).pdf | 1.07 MB |
Global Health Watch 4

Global Health Watch 3



Global Health Watch is coordinated by :